Volume 386, Issue 9992, 1 August 2015
Volume 386, Issue 9992, 1 August 2015
WORLD REPORT In July, 1965, Medicare, America’s landmark national health insurance programme, became law. Today, it covers 55 million people. Susan Jaffe, The Lancet’s Washington correspondent, reports.
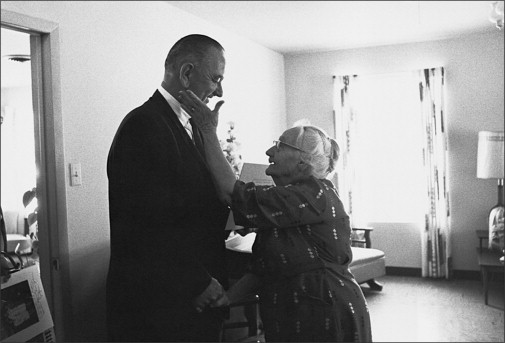
An American woman thanks President Lyndon Johnson for Medicare, April, 1965.
Richard Troeh joined a very busy solo family medicine practice in 1966 but even with two doctors, their offi ce in Independence, Missouri, seemed just as hectic. The year before, President Lyndon Baines Johnson came to town to sign the Medicare legislation into law at the Truman library. Former President Harry Truman—an advocate of national health insurance since the 1940s—and his wife attended the event and were among the fi rst Americans to receive Medicare cards.
50 years later, the Social Security Amendments of 1965 provide health care for 55 million people older than 65 years or disabled receiving Medicare and nearly 73 million low-income adults, children, pregnant women, and people with disabilities receiving Medicaid, an optional programme also created under the same law.
And in the process, the government programmes have transformed health care in the USA. Medicare is the nation’s largest single purchaser of health care, consuming 14% of last year’s federal budget, or US$505 billion. And it also has a fiercely loyal following that opposes efforts to cut benefits. Speaking earlier this month at the White House Conference on Aging, President Barack Obama drew laughs when he said, “And now we’ve got [protest] signs saying, “Get your government hands off of my Medicare”. [Continued in full text or PDF ] [listen to podcast here]

 period for these private drug and Advantage plans for 2016 starts Thursday and runs through Dec. 7.
period for these private drug and Advantage plans for 2016 starts Thursday and runs through Dec. 7.

 t been easy—surviving two Supreme Court challenges, nearly done-in by embarrassing technical glitches, and more than 50 congressional votes attempting to dismantle it. But its troubles are not yet over: enrolling new beneficiaries “is going to be tougher than last year”, warned Health and Human Services (HHS) Secretary Sylvia Mathews Burwell.
t been easy—surviving two Supreme Court challenges, nearly done-in by embarrassing technical glitches, and more than 50 congressional votes attempting to dismantle it. But its troubles are not yet over: enrolling new beneficiaries “is going to be tougher than last year”, warned Health and Human Services (HHS) Secretary Sylvia Mathews Burwell.